There is a delicate relationship between movements of the lower extremity and associated stability of the pelvis and spine.
A link has even been uncovered between low back pain and the subsequent development of cervical symptoms, suggesting a chain of reactions throughout the musculoskeletal system.1
For a healthy patient, we must help establish patterns of joint and muscular interactions that function automatically, from head to toe. However, since proper vertebral function is affected by simple gait,excessive pronation, any cause of leg length inequality, or uncoordinated muscle patterns may be overlooked obstacles in the proper treatment of subluxations and pain syndromes, including sciatica. 2
Understand the pattern
Guyton refers to one type of predictable joint and muscular activity as “sensory engrams for motor control.” The sequence for recruiting muscles during routine activities, like walking, can be considered recorded or “burned” into the sensory system for rapid retrieval and “replayed” by the motor system. Rather than reinvent the neurological commands necessary for repetitive movements, the necessary “pattern is located in the sensory part of the brain, and the motor system merely ‘follows’ the pattern.”3
Unfortunately, the sensory system does not discriminate between healthy and pathological engrams, it simply records frequently occurring patterns of activity or postures.
That should help you understand the return of patients’ postural faults, despite your best adjustments. When a patient presents with generalized hip and sacroiliac pain, including true sciatic nerve irritation, it is very likely that he/she has a habit (crossing the legs, for example) or postural distortion that contributes to her subluxation patterns.
All too often, the underlying cause of the dysfunction is distant from the site of pain, like altered foot biomechanics, or cervical spine dysfunction. In this case, unless a healthier engram is established, the subluxation patterns will return.
The impact of abnormal gait
When patients don’t respond to your chiropractic care as expected, look for a collapse in the arches of the feet or for habitual posture distortions. A more recent study reinforces that “there are small, but important, inter-segmental movements of the spine during gait.”4
Abnormal motion initiated by excessive or restricted joint interactions of the feet and lower extremities will eventually interfere with normal spinal-pelvic motions and can lead to pain syndromes.
A common dysfunctional lower-extremity pattern is hyperpronation producing excessive internal rotation of the entire lower extremity. The increased rotational forces are
transmitted into the pelvis and hip region where the primary antagonist is the piriformis muscle.
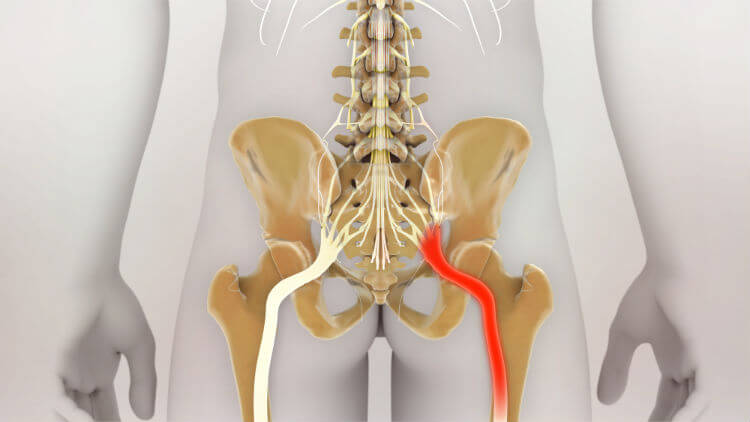
There are at least two mechanisms where piriformis irritation can contribute to sciatic nerve irritation. First, spasm or
hypertrophy can directly irritate the fibers forming the sciatic nerve, as they pass through the belly of the piriformis muscle.5 Second, when irritated, the piriformis can release inflammation by-products that have been shown to chemically irritate the nerve fibers.6
Leg length inequality matters
Piriformis syndrome is only one example of the possible consequences of poorly supported arches. The leg length inequality (LLI) that can also result from hyperpronation can potentially irritate any weak link further up the kinetic chain, whatever that may be for your particular patient.
LLI is categorized as either structural or functional. Both types result in similar adaptations throughout the musculoskeletal system and are difficult to distinguish without extensive evaluation. Because of adaptation, patients may be unaware of their LLI. The first indication is often found on a routine, weight-bearing, A-P lumbopelvic radiograph in a chiropractic office.
Without a specific history for structural LLI, including fracture, neoplasm, or degenerative arthritis, a conservative approach begins with a thorough evaluation for unilateral hyperpronation or supination. Harrison states that “asymmetrical pronation has the effect of producing pelvic tilt…” and Rothbart and Estabrook conclude that hyperpronation is the most common cause of a functional LLI. 7,8
An initial A-P pelvic X-ray, with the patient standing barefoot, will provide a baseline. For an indication of the functional component of the measured LLI on the radiograph, compare your results using a navicular drop test.
Whenever your patient presents with pelvic unleveling and a functional short leg as a result of hyperpronation, support the entire foot with a custom-made orthotic without a lift, initially. Ideally, the LLI should be reduced to less than 10 mm (shown clinically to be significant for DJD) and preferably less than 5 mm (associated with back, hip and leg
pain). 9,10,11 If not, it is very likely that bringing the
LLI within 5mm will require the use of a lift, in conjunction with the orthotic.
Bilateral arch collapse may not produce a LLI but it favors flexion of the entire pelvis. The lumbar lordosis is increased, putting excessive pressure on the posterior spinal joints. The patient is not only likely to experience
increased facet irritation, but also to compensate with an increase in the thoracic kyphosis and with anterior weightbearing of the cervical spine. This postural presentation of the classic chiropractic patient sets the stage for injury, fatigue, and degenerative arthritis.
The body’s overall stability is greatly reduced, and it requires greater effort to simply remain standing. In fact, Cailliet says that for an inch of abnormal anterior cervical translation, there is a corresponding ten-fold increase in cervical spine muscle effort.12
This is a clear example of uncoordinated muscle patterns, where it might be tempting to rehabilitate only those muscles near the spine. Recent emphasis has shifted to balancing activity among groups of
muscles for the prevention and management of pain syndromes, since muscle dysfunction can either be a direct source of pain or complicit in pain referral. 13
Agonists vs. antagonists
There is a natural strength difference between agonists and antagonists, which sets a stage for muscular involvement. Generally, trunk extensors are stronger than flexors.14
Furthermore, it is understood that some muscles are prone to weakness and others to tightening when injured . Jull and Janda give the example of degenerative hip pathology that presents with tightness in the iliopsoas and hip adductors but with atrophy and weakness of the glutei.

“These muscle reactions are not random but are consistent and it is considered that such typical responses of muscle tightness and weakness occur throughout the whole muscular system.”15
Combining the effects of negative engrams with the tendency of certain muscles to react in predictable but opposite patterns, it becomes obvious how important it is to evaluate our patients’ global posture.
The most effective adjustments may be diminished through uncooperative muscle activity.
Improperly functioning muscles also affect normal transmission of proprioceptive feedback, another mechanism in the kinetic chain relationship.
“The importance of adequate sensory input, proprioceptive control and proper function of sensorimotor integration has probably been underestimated in the pathogenesis of low back pain…For this reason, proprioceptive facilitation techniques should be included in the therapeutic programs for those suffering from low back pain syndromes and postural defects.”15
Chiropractic adjustments of the spine improve proprioceptive input by normalizing joint alignment and muscle tonus. Furthermore, because the feet contain approximately one quarter of all the body’s joints and, therefore, a concentration of proprioceptive fibers, it becomes logical to conclude that support of the postural foundation using custom-made orthotics will enhance balance and muscle coordination. In fact, this was the conclusion reached during research involving custom orthotics, published in JMPT.16
The reason a diagnosis of true sciatic nerve irritation can be difficult to reach is the comprehensive nature of the structures involved in the pathogenesis of this condition. Only chiropractors are equipped to address the several components of joint subluxation, muscular imbalance, and sensorimotor feedback errors.
However, unless a global approach is taken for this and most other conditions, results will be short lived. Successful treatments will combine specific adjustments to counteract the patterns of joint dysfunction, combined with rehabilitation of specific muscle groups and support for deficient structures, including the feet and lower extremities.
Download a free sciatica poster here.
References
1. Horal J: The clinical appearance of low back disorders in the city of Gothenburg, Sweden. Acta Orthop Scand suppl 118:15, 1969.
2. Yekutiel MP. The role of vertebral movement in gait: implications for manual therapy. J Man Manip Ther 1994; 2:22-27.
3. Guyton AC. Textbook of Medical Philosophy, 6th ed. Philadelphia: W.B. Saunders Company, 1981.
4. Sychewska M, Oberg T, Karlsson D. Segmental movements of the spine during treadmill walking with normal speed. Clin Biomech 1999; 14:384-388.
5. Cox JM. Low Back Pain: Mechanism, Diagnosis and Treatment, 5th ed. Baltimore: Williams & Wilkins, 1990.
6. Steiner C et al. Piriformis syndrome: pathogenesis, diagnosis, and treatment. J Am Osteopath Assoc 1987; 87:318.
7. Harrison, D. et al. CPB, Vol. 4. 1998.
8. Rothbart BA, Estabrook L. Excessive pronation : a major biomechanical determinant in the development of chondromalacia and pelvic lists. JMPT 1988; 11:373-379.
9. Giles LGF, Taylor JR. Lumbar spine structural changes associated with leg length inequality. Spine 1982; 7:159-162.
10. Giles LGF, Taylor JR. Low back pain associated with leg length inequality. Spine 1981; 6:510-521.
11. Friberg O: Clinical Symptoms and Biomechanics of Lumbar Spine and Hip Joint in Leg Length Inequality. Spine 1983, 6(6): 643-650.
12. Cailliet R. Neck and Arm Pain. Philadelphia: F.A. Davis, 1981.
13. Lewit K: Manipulative Therapy in Rehabilitation of the Motor System. Butterworth, London, 1985.
14. Langrana NA, Lee CK, Alexander H, Mayott CW: Quantitative assessment of back strength using isokenetic testing. Spine 9:287, 1984.
15. Jull GA, and Janda V. Muscles and motor control in low back pain: assessment and management. In Physical Therapy of the Low Back. Churchill Livingstone, New York 1987.
16. Stude DE, Brink DK. Effects of nine holes of simulated golf and orthotic intervention on balance and proprioception in experienced golfers. J Manip Physiol Ther 1997; 20:590-601.
Related Posts
 Integrative Therapeutics to sponsor webinar on hormone therapy prescriptions
Integrative Therapeutics to sponsor webinar on hormone therapy prescriptions- Is your Medicare enrollment record up to date?
- ACA Engage 2026 to feature new CE, social opportunities
- Palmer College of Chiropractic launches 20/20/20 research campaign
- Parker Seminars Dallas Features ‘Shark Tank’ Star on Oct. 1-3





