
Because of its mobility, the shoulder is one of the most at-risk joints in the body. It’s no wonder chiropractors often see shoulder injuries; shoulder pain is reported in 14.7 per 1,000 patients per year with a lifetime prevalence of up to 70%, and a recurrence rate as high as 25%.[1] These injuries can develop after a major incident, minor movements, or seemingly out of nowhere – and they become more prevalent with age.
Treatments for shoulder injuries are typically multi-faceted and can range from adjustments to NSAIDs to surgery in severe cases. Super pulsed laser therapy offers a non-invasive way for chiropractors to relieve pain and inflammation and accelerate the recovery process, allowing patients to get back to normal activities faster than traditional methods that may come with risks or side effects.
Keep reading to find out how one chiropractor used a comprehensive super pulsed laser therapy protocol combined with Activator Methods to prevent a case of frozen shoulder in a patient, reducing her recovery time from 18-24 months down to just 4 weeks.
Combination of Photobiomodulation and Chiropractic Care for the Management of an Acute Shoulder Injury
Author: Brian Fitzpatrick, DC, CLS
Condition
The patient presented with an acute supraspinatus injury and showed signs of early painful phase of adhesive capsulitis. The classic presentation of adhesive capsulitis includes localized shoulder pain and restricted active and passive range of motion and follows 3 phases: painful, stiffening, and thawing. Adhesive capsulitis is more prevalent in women between the ages of 40-70 and often occurs after surgery or an injury. Common treatments include NSAIDs and physical therapy, including stretches. The prognosis is often 18-24 months for complete recovery.
Purpose
The patient’s demographic and occupational history suggested that adhesive capsulitis was a high probability, if left untreated. Both photobiomodulation and chiropractic care have been shown to be effective in treating acute musculoskeletal conditions.[2] For this case study, the two treatments were applied together, utilizing Activator Methods for chiropractic protocols and the Priority Principle for phototherapy protocols. The patient was assessed subjectively (VAS) and objectively (range of motion).
Patient Profile
A 59-year-old female patient came into the office with a new complaint that started one day prior when she woke up at 3:30 am with severe right shoulder pain after leaf blowing the day before. She remarked that her sleep was severely disturbed, and she was barely able to move her right shoulder. She visited her family doctor earlier that day and was told to continue taking Advil and seek out physical therapy. The patient presented with no co-morbidities and noted that her greatest concern was moving her right arm, given her custodial occupation requires her to reach above her to head to wipe and scrub walls.
Assessment
Further questioning and examination revealed that the patient’s main complaint was localized to the right glenohumeral joint capsule and lateral supraspinatus insertion and elicited 9/10 pain with any movement beyond 10-20 degrees in any direction. Orthopedic tests of Apley’s, Dugas, and Impingement were positive with limited range of motions and localized pain to the right glenohumeral joint capsule. Inflammation was noted around the right glenohumeral joint capsule and supraspinatus insertion and hypertonicity in the right trapezius and cervical paraspinal musculature.
Figure 1: The following right shoulder ranges of motion were measured, each resulting in severe shoulder pain.

Intervention
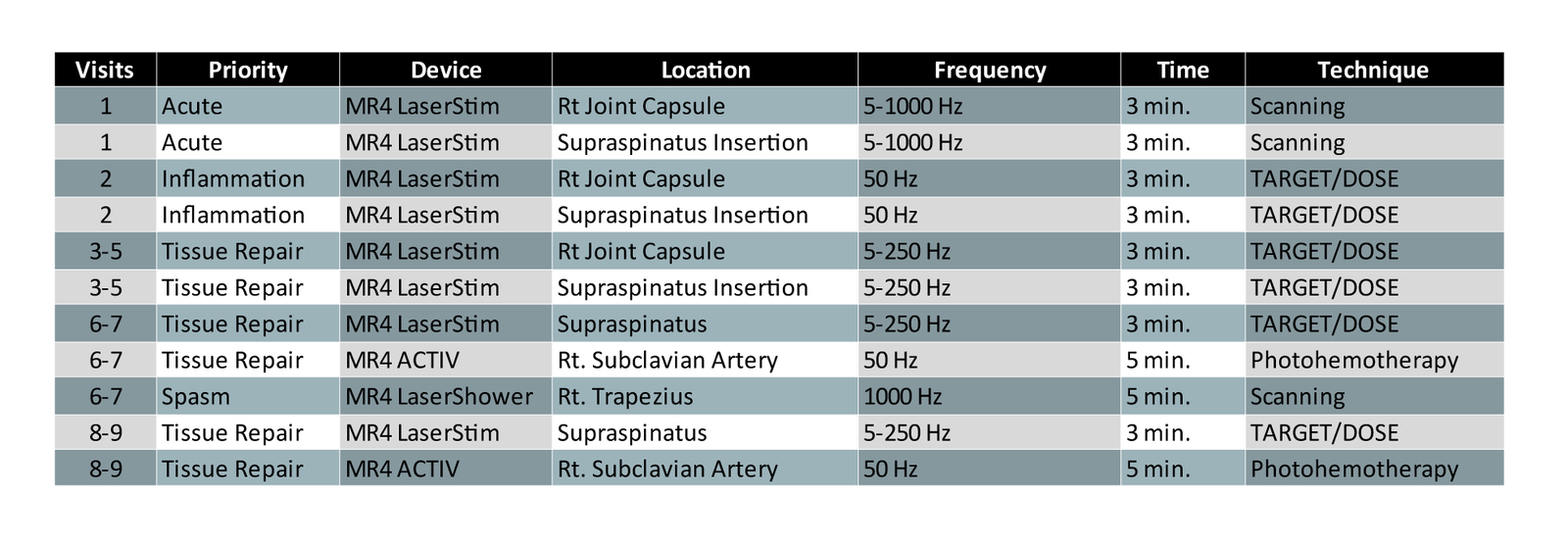
A treatment plan was constructed with a treatment frequency of 3 times a week for 2 weeks; then 2 times a week for 1 week; and then 1 time a week for 1 week (totaling 9 visits over 4 weeks). Each visit consisted of an Activator Method basic scan and additional testing to the right glenohumeral and rotator cuff regions. Chiropractic adjustments were performed as indicated. Phototherapy with combination of super pulsed laser and light-emitting diodes (Multi Radiance Medical) was also utilized each visit by applying the concepts of the Priority Principle.
Outcomes
On each visit, the patient’s right shoulder abduction and pain associated with that movement was measured. By the third visit, the inflammatory process had resolved, resulting in no more sharp pain with end range of motion and was replaced with a mild to moderate dull ache. Pain-free range of motion increased from 10 degrees to 160 degrees within the first week and then plateaued until the end of the treatment phase (Figure 2).
The patient reported being able to return to work without restrictions by the second week of care and reported no exacerbations during the 3rd and 4th weeks of care.

Discussion
This case illustrates the importance of when treatment is delivered in shoulder injuries. By treating the patient within 48 hours of the initial injury, the Rescue Protocol (5-1000Hz for 3 minutes) from the Priority Principle was able to be used on the first visit, followed by utilizing the Inflammation Principle (50 Hz for 3 minutes) on the 2nd visit to resolve acute inflammation before the tissue had a chance to move into the subacute and chronic phases. Due to this, by the 3rd visit (5th day since the injury onset), the patient reported that pain has decreased from a 9 to a 3 out of 10 and right shoulder abduction has increased from 10 to 160 degrees and was able to return to full work duties the following week.
Secondary adhesive capsulitis is usually preceded by some sort of trauma or surgery that forced immobilization of the shoulder. By addressing the inflammation first, the inflammatory nociceptive pain subsided and shoulder range of motion was restored before the stiffening phase could begin.
While both chiropractic adjustments[3] and low-level laser therapy[4] have been shown to be effective at treating adhesive capsulitis after the stiffness phase, the patient’s lifestyle modifications and prognosis are better if treated earlier.
From the 3rd visit on, the patient presented with no signs of acute injury (swelling, inflammation, significant pain, or spasm) so the Tissue Repair Principle (5-250Hz for 3 minutes locally and 50Hz for 5 minutes at the subclavian artery) was used to address the functional movement deficits until full pain-free range of motion was restored and the patient was discharged.
By addressing the shoulder injury early and following through with care until there were no residual symptoms, the patient has had no right shoulder complaints for 3 years.
Learn more about laser therapy for chiropractic in the Laser Therapy Resource Center.
About the Author
Brian Fitzpatrick, DC, 2007 valedictorian from Palmer College of Chiropractic where he received the Virgil V. Strang Philosophy Award as well as the John Connolly Memorial Award for scholarship and involvement in Palmer and community organizations.
Dr. Fitzpatrick is an Associate Clinical Instructor for Activator Methods, a Certified Laser Specialist, and a member of the Medical Advisory Board for Multi Radiance Medical. He practices at Fitzpatrick Family Chiropractic in Solon, IA.
References:
- Cadogan, A., Laslett, M., Hing, W.A. et al. A prospective study of shoulder pain in primary care: Prevalence of imaged pathology and response to guided diagnostic blocks. BMC Musculoskelet Disord 12, 119 (2011). https://doi.org/10.1186/1471-2474-12-119
- Cotler, H. B., Chow, R. T., Hamblin, M. R., & Carroll, J. (2015). The Use of Low Level Laser Therapy (LLLT) For Musculoskeletal Pain. MOJ orthopedics & rheumatology, 2(5), 00068. https://doi.org/10.15406/mojor.2015.02.00068
- Polkinghorn B.S. Chiropractic treatment of frozen shoulder syndrome (adhesive capsulitis) utilizing mechanical force, manually assisted short lever adjusting procedures. J Manipulative Physiol Ther. 1995;18 (2):105–115.
- David Ip and Nga-Yue Fu. Two-year follow-up of low-level laser therapy for elderly with painful adhesive capsulitis of the shoulder. J Pain Res. 2015; 8: 247–252.
