By Daniel J. Bourassa, DC
Abstract
Low level laser therapy (LLLT) has found increasing clinical acceptance in cosmetic body contouring and spot fat reduction. This study examined whether LLLT using 630-680 nm, 150 mW shower arrays and single 40 mW diode laser radiation sources produced significant clinical effect for this purpose. A review of clinical results was made of 311 patient records collected over a 26 month period that underwent LLLT for cosmetic purposes to the abdominal/torso area. Clinical results showing measured abdominal reduction are presented. Overall, 130 patients in 6 session and 12 session groups achieved average sustained losses of 6.55 cm and 11.04 cm corresponding to an average girth reduction of 0.48 -0.55 cm per session. With weight loss of a minimum of 0.68 kg per week, results averaged 9.0 cm for the 6 session group and 16.1 cm for the 12 session group corresponding to an average girth reduction 0.67-0.75 cm per session. Initial session losses of 253 patients averaged 2.79 cm or 1.4 cm in girth reduction. 75.2% were able to sustain at least 4 cm or more loss in 6 or more sessions. Effects of variations in protocol to include number treatments, session time, total laser time per treatment, weight loss effects, use of topical fat reduction creams as well as potential topics for further study are discussed. Based on the review of patient results, it would appear that LLLT can be an effective therapy for body contouring and spot fat reduction.
Introduction
The use of low level laser radiation therapy (LLLT) in the 600-900 nm wavelength spectrums is in common usage in musculoskeletal therapy and wound healing. Karu has discussed the photo-biological action that occurs in the enhancement of cellular mechanisms through activation of the respiratory chain leading to physiological changes to the cell. (1)
The application of LLLT to cosmetic fat reduction is relatively new and began with low powered laser assisted lipoplasty. Neira, et al. demonstrated by magnetic resonance imaging that 635 nm LLLT induced changes in density and organization of the subcutaneous fatty layer after 4 and 6 minutes. (2) It was also demonstrated that 635 nm LLLT results in liquefaction of contained fat and its migration out of the fat cell in as little as 4 minutes (80%) and near total emptying of the fat cell (99%) in 6 minutes using tumesent technique. (3) These changes were consistent with an earlier study demonstrating changes by examination with electron microscope to include transient micropore formation in the fat cell walls. (2) (3)
It is known that LLLT is associated with stimulation of cyclic adenosine monophosphate in cells. (4) (5) Neira, et al. points out that “ The adipocyte membrane is activated by different concentrations of cyclic adenosine monophosphate that stimulate, in turn, cytoplasmic lipase that triggers conversion of triglycerides into fatty acids and glycerol, both elements that can easily pass through cell membranes.” (3) Results withouttumescent technique at six minutes laser exposure was comparable to four minutes with tumescent technique. They conclude that “ The laser facilitates the releasing of fat and contributes to the disruption of fat pannicles, allowing the fat to go from inside to outside the cell and placing it in the interstitial space.” (3) Other researchers found no consistent observations of adipocyte disruptions. (6)
Most available reports concerning the use of LLLT for body contouring and spot fat reduction are anecdotal. There are few available Western published clinical studies regarding use and effectiveness of LLLT as a primary therapy in this area. Caruso-Davis, et al. at the Pennington Biomedical Research Center/Louisiana State University System have researched the Lapex 2000 as a LLLT for body contouring and spot fat reduction and compared it to mesotherapy. They also found evidence that LLLT creates pores in adipocytes but concluded only free fatty acids are released and not glycerol. (7) They have earlier reported that LLLT using the Lapex 2000 “gives significant girth loss that is maintained over repeated treatments and is cumulative over 4 weeks of 8 treatments.” (8)
The purpose of this study is to present a review of clinical results on body contouring and spot fat reduction of the abdominal area compiled from 311 patient records collected over a 26 month time frame beginning in 2007 using continuous LLLT in the 630nm~680nm wavelength from AlGalnP semi-conductor laser diodes. This review is primarily focused on results observed from 1st session treatment as well 6 and 12 treatment programs along with the effects of variations in protocol to include application time and number of applications per treatment session, total laser time per treatment session, and weight loss.
Materials and Methods
Meridian Medical’s LAPEX 2000 LIPOLASER is a non-invasive digital semiconductor Class IIIB laser device utilizing 2 multi-probe paddles and 2 EN probes with simultaneous and independent management of outputs for connecting paddles and probes. It was originally developed to treat carpal tunnel syndrome and then modified for cosmetic spot fat reduction. The lasers are AlGalnP semiconductors diodes with continuous output in the 630-680 nm wavelengths. The multi probe paddles are multi-beam shower method high power lasers composed of 4 in line laser arrays in rated at 150mW+/- 20%.The EN probes are single high power laser arrays rated at 40mW+/-20%.


 All patients underwent pretreatment consultation and screening to include history, potential risk factors, as well as physical assessment to include vital signs, sex, age, height, weight, body mass index, body fat % by bio-impedance method, and fitness index. This pre-treatment consult explained the Lapex 2000 treatment, lipolaser procedures, expectations and risks, and physical examination of areas to be treated. All patients were advised that proper diet and exercise were recommended for best results in metabolizing released fat per manufacturer’s guidelines. All patients signed informed consent and consent forms for release of pictures and medical information.
All patients underwent pretreatment consultation and screening to include history, potential risk factors, as well as physical assessment to include vital signs, sex, age, height, weight, body mass index, body fat % by bio-impedance method, and fitness index. This pre-treatment consult explained the Lapex 2000 treatment, lipolaser procedures, expectations and risks, and physical examination of areas to be treated. All patients were advised that proper diet and exercise were recommended for best results in metabolizing released fat per manufacturer’s guidelines. All patients signed informed consent and consent forms for release of pictures and medical information.
The LAPEX 2000 LIPOLASER was applied topically (direct contact) on skin of the abdomen and torso to areas where undesired fat was present.
Treatment protocols consisted of the following:
*The recommended treatment protocol for the LAPEX 2000 was twice weekly with a minimum 48 hour between subsequent treatments.
*Number of treatment varied from 1 application to 24 applications. The most frequent number of treatments was for 6-12 treatments (3 to 6 weeks). Measurements were taken at every 3-4 sessions and using 2 measurements (predominantly 1″ above and below the umbilicus) and at completion of treatment. Spot photos were taken as pre and post completion of treatment sessions.
*The treatment time was varied between 30-50 minutes per session with application times varying from 6 to 10 minutes.Pre and Post 12 session loss +/- 0.68 kg from base starting weight (12cm loss)
*Abdominal and torso treatment is followed by 10 minutes on a whole body vibration machine.
*Patients were encouraged to participate in cardio activity and/or exercise program within 24 hrs after the treatment to stimulate the muscles to use the free fatty acids as energy.
*Patients were advised to drink plenty of water following the treatment.
*Patients were encouraged to modify diet to achieve a minimum of 0.68 kg (1.5lbs) per week of weight reduction. No specified diet was given.
*Patients with over 30% body fat were encouraged to join and participate in a supervised weight loss program, not affiliated with this office, to aide in weight loss.
*Nutritional supplements, including Irvingia based products, depending on individual requirements were also recommended to some patients to help augment natural metabolic function to normal levels to aid weight loss.
 Results
Results
311 patients, consisting of 272 females and 39 males ages 18 to 81, underwent from 1 to 24 laser treatments to the abdominal and torso areas. 170 patients had 6 or more treatment sessions.
Measured loss from a single first session treatment sample of 253 patients averaged 2.79cm (range: 0cm-9cm) or 1.4cm in girth reduction covering all application times. For 6, 8 and 10 minute application times the first session measured loss averaged 3.0cm (range: 0.5cm-9cm) or 1.5 cm girth reduction; 3.5cm (range: 1.5cm-6cm) or 1.8cm girth reduction; and 2.63cm (range: 0cm-6.5cm) or 1.3cm girth reduction respectively.
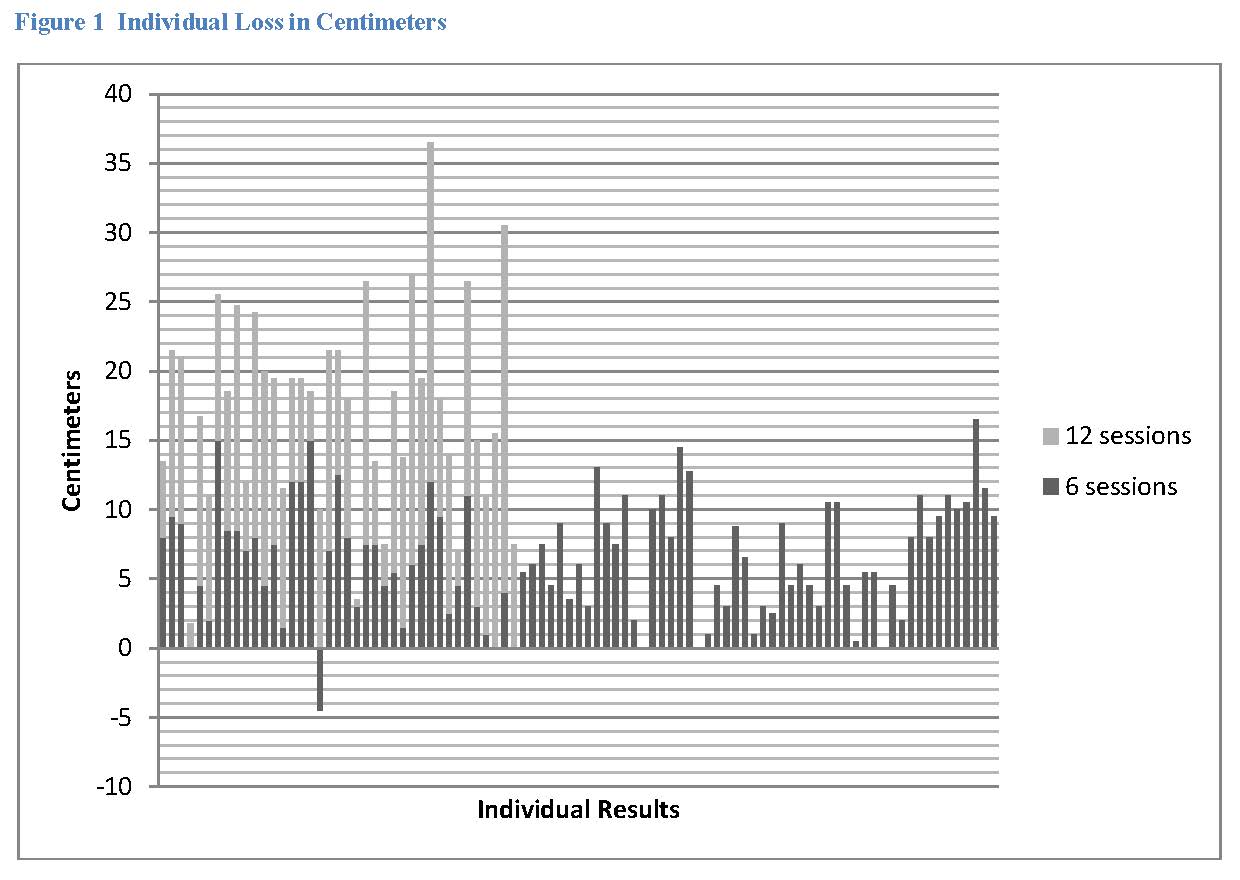
The study sample with either 6 or 12 sessions consisted of 130 patients. Of this sample, 91 patients had 6 sessions with an average sustained loss of 6.55cm (range: -4.5cm-16.5cm) and of 39 patients that had 12 sessions an average sustained loss of 11.04cm (range: 0.5 cm-26.5 cm) was achieved. This results in an average girth reduction of 0.46-0.55 cm per session. Average weight loss for the 6 and 12 session groups was 0.92 kg and 1.84 kg respectively.
Consistent with the Caruso, et al. study (8) parameters excluding weight loss as a variable, of the 50 patients in the 6 session group that lost 0 +/- 1.5 kg over the course of their treatment, the average sustained loss was 6.46 cm (range: 0 cm-15 cm). This results in an average girth reduction of 3.23 cm or 0.54 cm per session. In the 12 session group, the 14 patients that lost 0 +/- 1.5 kg averaged a sustained loss of 10.85 cm. This results in an average girth reduction of 5.43 cm or 0.45 cm per session. Patients that lost an average of 0.68 kg/week for both the 6 and 12 session treatment groups averaged a 9.0 cm (range: 3 cm-12 cm) and 16.1cm (range: 7.5 cm-26.5 cm) respectively.
This results in an average girth reduction of 4.5 cm or 0.75 cm per session for 6 sessions and 8.1 cm or 0.67 cm per session for 12 sessions with the recommended weight loss.
There were no adverse events reported among the 354 patients. 42 (24.8%) of 170 patients experienced less than 4cm sustained loss after 6 or more sessions. 14 patients (8%) experienced no loss after 6 or more sessions. Only 6 patients (2.3%) of the 253 patients measured for their first session experienced no loss from the treatment.
Discussion
LLLT application for body contouring and spot fat reduction has found increased acceptance as new cosmetic therapy. Glowing advertisements and celebrity endorsements abound yet there are limited studies available for clinicians and patients on which to base their choices for treatment.
In assessing the results available in this study sample of 311 patients that received treatment to the abdominal/torso area, there were several observations as well as questions raised regarding both the present protocols and available delivery system design of the Lapex 2000. What appears evident is that 630 nm-680 nm LLLT is a viable therapy choice for body contouring and spot faction reduction delivering excellent results for a majority of patients.
Using Caruso, et al. criteria for +/- 1.5 kg of baseline weight and 30 minute sessions 2x/week for 3 weeks; it was found that three 10 minute applications produced an average of 4.72 cm loss (with a range of 0-12.5 cm total loss) and an average girth reduction 0.39 cm per session; for five 6 minute applications the measured loss was 8.40 cm (with a range of 0.5-15 cm total loss) and an average girth reduction 0.70 cm per session. Increasing the total time to 48 minutes, i.e. eight 6 minute applications, improved the outcome to an average of 12 cm (with a range of 9.5 – 16.5 cm) and an average girth reduction 1.0cm per session. (Fig 1)
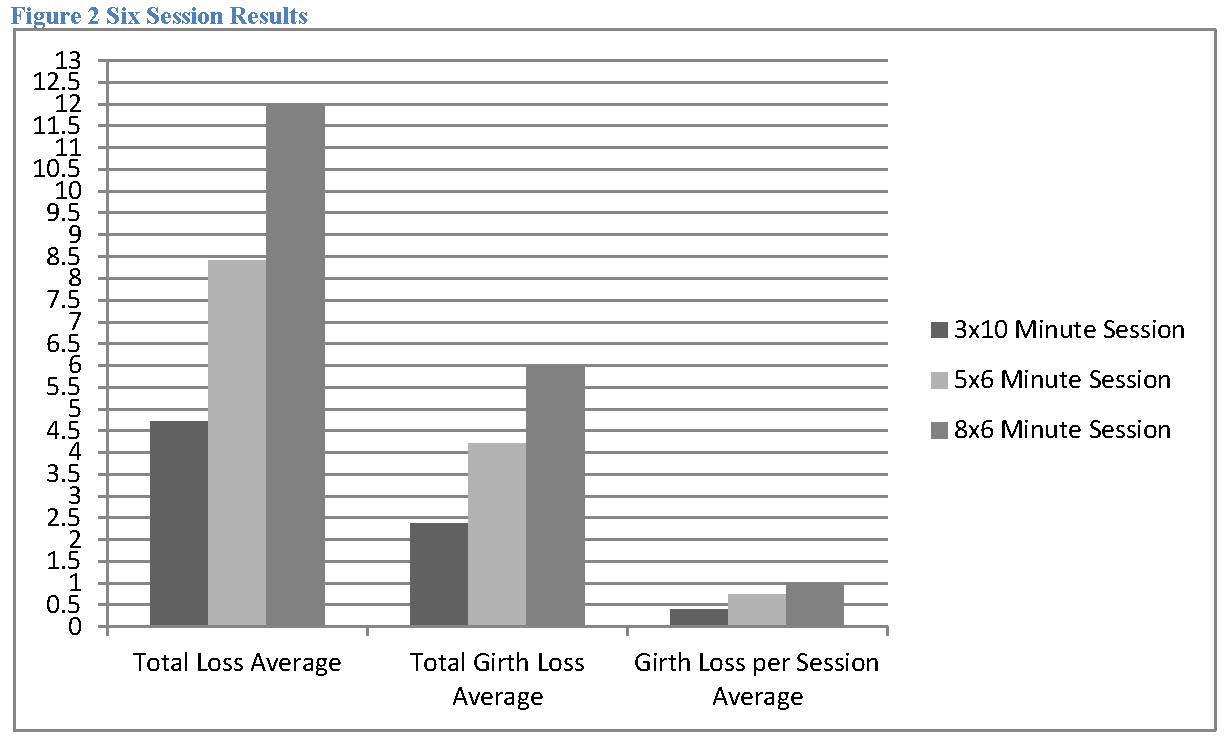
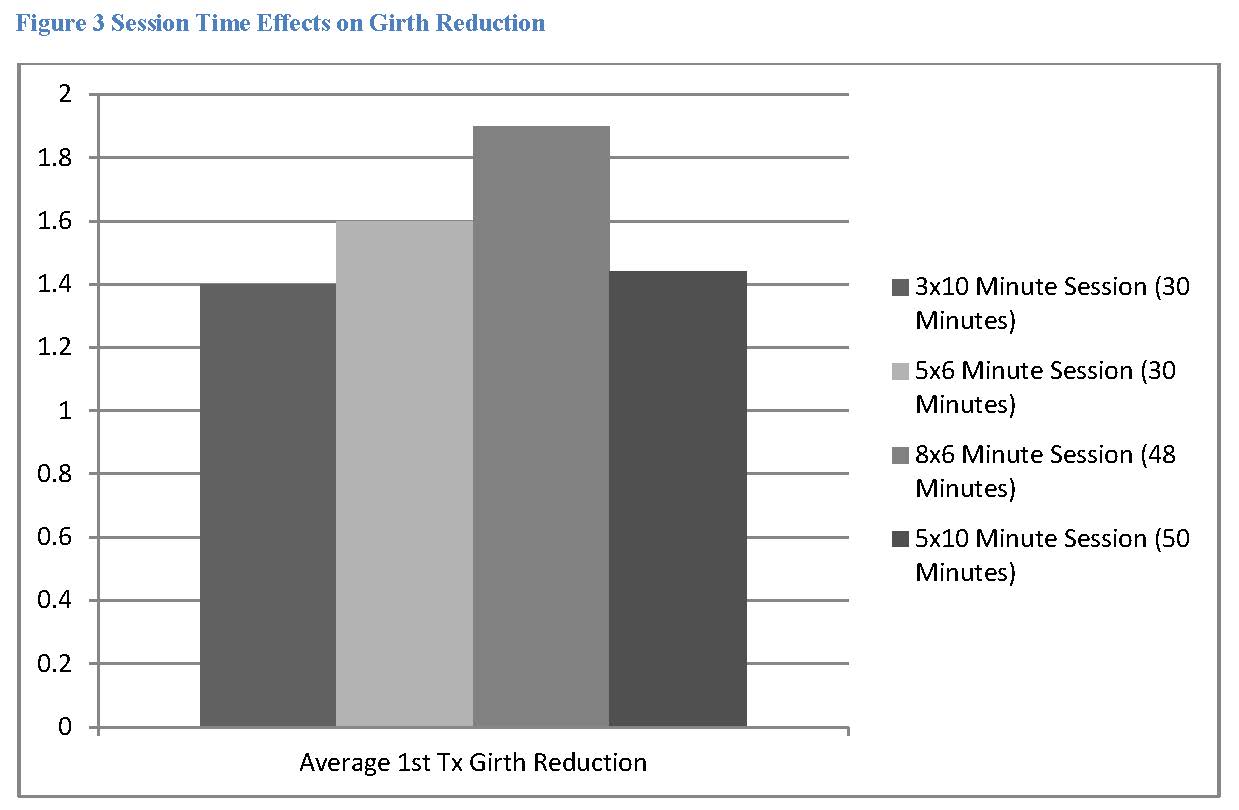
Additionally, first treatment pre and post measurements of patients averaged losses of 2.83cm (1.4cm girth reduction) for 10 min group and 3.17cm (1.6cm girth reduction) for 6 min group with 30 minute total time. Increasing the 6 min group to 48 minutes per session averaged 3.83cm (1.9cm girth reduction). It would appear, simply increasing time does not seem to translate as well into measured loss compared to shorter application and greater percentage cell coverage in that increasing the 10 minute application to 5 (i.e. 50 minutes) yielded only 2.88cm loss (1.44cm girth reduction) for the first session compared to 2.83 (1.4cm girth reduction) for 30 minutes. (Fig 2)
The improvement in girth reduction with shorter application times of 6 (3.5 J/ cm2 at 12.5mm) and 8 (4.6 J/ cm2 at 12.5mm) minutes raises questions regarding photoreceptor saturation consistent with Arndt-Schultz law with longer exposure times as being less effective. The best single session results were achieved with eight 6 minute applications but not necessarily over the length of 6-12 sessions again suggesting photoreceptor burn out as well as free fatty acid elimination problems. It also seems apparent that the greater number of fat cell exposure by more applications in a single session also contributes to greater girth loss. Controlled studies are needed to clarify optimum dosing to effect optimum results from treatment.
It is not known precisely why consistent cumulative loss is not seen in subsequent sessions. However, it has been observed that measurable losses occurs during each session. Pre-identified metabolic problems were present in a majority of patients that did poorly over several sessions to include controlled diabetes and hypothyroidism. Along with metabolic problems, these patients also gained weight or failed to lose an average 0.68 kg week during treatment. It would seem to follow that the released free fatty acids are not consistently removed from treatment area or body and are redeposit back into lipocytes, or are replaced by dietary free fatty acids in those patients that responded poorly to multiple sessions. This is an area for further research.
Additionally, it must be considered that photoreceptors damage or inhibition may be occurring in subsequent sessions or that 48 hours is inadequate to allow for photoreceptor00.20.40.60.811.21.41.61.82Average 1st Tx Girth Reduction3x10 Minute Session (30 Minutes)5×6 Minute Session (30 Minutes)8×6 Minute Session (48 Minutes)5×10 Minute Session (50 Minutes)recovery in some cases. It is known that positive photocontrol of cellular metabolism occurs in a narrow dose range and as dose increases, photoreceptors are damaged and the effect decreases. (4) Karu has also pointed out that LLLT biological effects on cells have been observed over 6-7 days post irradiation. (4) The results also suggests maximum therapeutic benefit is achieved in shorter and more coverage area application time than the three to four 10 minute applications per session (30 -40 minutes sessions) recommended by the manufacturer. Further research is needed to determine optimum interval, duration, and frequency.
Results observed in this review are consistent with Caruso, et.al. for per session average girth loss (0.39-0.54 cm vs. 0.4-0.5 cm) when using manufacturer’s protocols but significantly improved using shorter application times on average by up to 50% (0.70 cm) and greater area coverage with increased time by up to 115% (1.0 cm).
Lifestyle changes are recommended to include diet modification/restriction and moderate exercise by the manufacturer to facilitate metabolization of the released free fatty acids. While it does not appear that weight loss is a requirement for significant girth reduction in normal metabolic patients; those achieving a 0.68+ kg weekly weight reduction increased girth loss by an average of 31% and 40% for 6 session and 12 session treatment respectively. Correspondingly, due to increased risk of poor free fatty acid elimination weight reduction of a minimum of 0.68 kg should be strongly encouraged for patients with pre-identified metabolic problems. These patients may require a supervised weight loss program or other medical management to achieve maximum benefit.Use of topical slimming creams, nutritional supplements, and Irvingia based weight loss supplements did not show significant difference in results from those patients that did not utilize them in this review. (+/-<1.0cm over 6 or more treatments)
References
1Karu T. Low-Power Laser Therapy. Biomedical Photonics Handbook. s.l. : Tuan Vo-Dinh CRS Press, 2003, p. Chapter 48.
2Neira R, Jackson R, Dedo D, Ortiz CL, Arroyave JA. Low-lovel Laser assisted lipoplasty appearance of fat demonstrated by MRI on abdominal tissue. 2001, The American Journal of Cosmetic Surgery, Vol. 18, no. 3, pp. 133-140.
3Neira R, Arroyave JA, Ramirez H, Ortiz CL, Solarte E, Sequeda F, Gutierrez MI. Fat liquefcation: effects of low-level laser energy on adipose tissue. 2002, Plastic & Reconstructive Surgery, Vol. 110, No. 3, pp. 912-922.
4Karu T. Molecular Mechanism of the Therapuetic Effect of Low-Intensity Laser Radiation. 1988, Lasers in Life Sciences (2)-1, pp. 53-74.
5Zungu IL, Hawkins Evans D, Abrahamse H. Mitochondrial responses of normal and injured human skin fibroblasts followwing low level laser irradiation-an in vitro study. s.l. : Photochemistry and Photobiology., 2009, Vols. 85(4): 987-96. Epub 2009 Feb 13.
6Brown SA. Rohrich RJ, Kenkel J, Young VL, Hoopman J, Coimra M. Effect of low level laser therapy on abdominal adipocytes before lipoplasty procedures. 2004 May, Plast Reconstr Surg. , pp. 1139^0:1796-804; discussion 1805-6.
7Caruso-Davis M, Guillot T, Yu Y, Mashtalir N, Bissoon L, Dhurandhar N, Greenway F. Mechanistic Studies for Local Fat Reduction. s.l. : Published in the journal Obesity 16(suppl. 1):S161, 2008, 2008. Presented at the NAASO Annual Scientific Meeting, Phoenix, AZ, October 3-7, 2008.
8Caruso MK, Guillot T, Vaccaro T, Yu Y, Williams D, Bissoon L, Greenway F. The Efficacy of the Lapex 2000 Lipo Laser in Body Contouring and Fat Reduction. Phoenix, AZ : Published in the journal Obesity 15(program Abstracts):A99, 2007, 2007. Presented at the NAASO Annual Scientific Meeting, New Orleans, LA, October 20-24, 2007.
Related Posts
 PayDC announces the release of billing, scheduling modules
PayDC announces the release of billing, scheduling modules- NUHS mourns passing of renowned alumnus N. Ray Tuck Jr., DC
- Northwestern Health Sciences University names Maria G. Boosalis as nutrition leader
- Kathy Mills Chang to host financial boot camps
- Life West Nebraska approved for international DC students





